Fracture fixation siugcxy is one of the main roles of the veterinary orthopaedic surgeon. however there is no single srugical technique that will be s:uccessful for stabilisation of all flractrue types Considerationofseveral key principles will aid the srugeon iS making correct decisiods witb tegard to the best way to stabilise any given fracture. Previously, aocurate reconsuuction of an fractrue fragments was considered to be the most important goal. however this often involves significant soft tissue dissection and disruption of blood supply. Nowadays. the imporr:ance of soft tissue preservation is seen as a critical part of fracture fixation surgery and techmques involving mmimal disruption at the fracture site generally result in much quicker healing tmies
If anatonucal reconstruction of the fractuie can be easily acbieved this creates a 'Ioad-sharmg'environment (fig l - scenario A below) with significant mechanical advantages and an increased area moment of mertia (AMI). AMI is a function of the bending stiffness of a construct Ifa fracture is non-reconstructable (fig l- scenario B below), this represents a 'non load-sbaring'situation with a lower AMI requiring a more rigid fixation system.
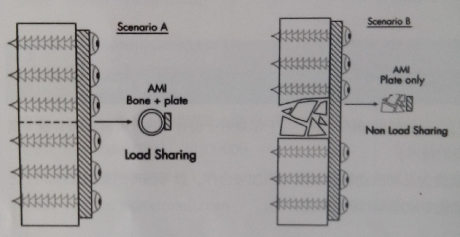
fig l:the conoept of load 8hartng and area moment of inertia (AMI)
In basic terms, fracture repair can be seen as a race between fracture healing and implanr failure. If the fracture does not heal quickly enough, eventually Lhe implants will fail by cyclical fatig ue or overload.
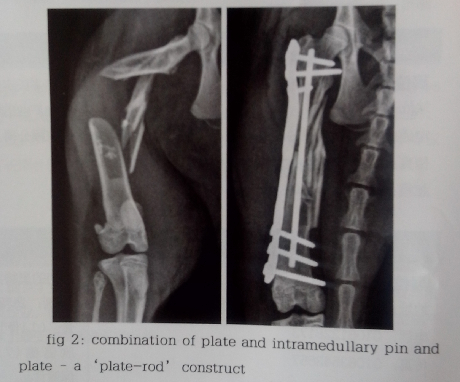
Most fractures fail due to bending stresses and the placement of an intramedullary pin is one of the easiest ways
to add significant strength to a fracture repair (fig 2).
In addition to minimally invasiw surgioal approaches preserving blood supply to the fracture sitn . the development of locking plate technology facilitates further preservation of the soft tissues and wcll as piuviciing additional suffiility,increasing the chanoes of a successful outcome.
If implant failure does occur, revision surgery invariably involves removal of the original implants, placement of more rigid fixation and placement of an autogenous cacicellous bone graft Bone grafts can oasily harvosted from tho proximal humerus or ilial wing and can potentially be 'extended 'with a variety of new bone graft substituLes, although autogenous graft remains the gold standard.
Pelvic limb lameness
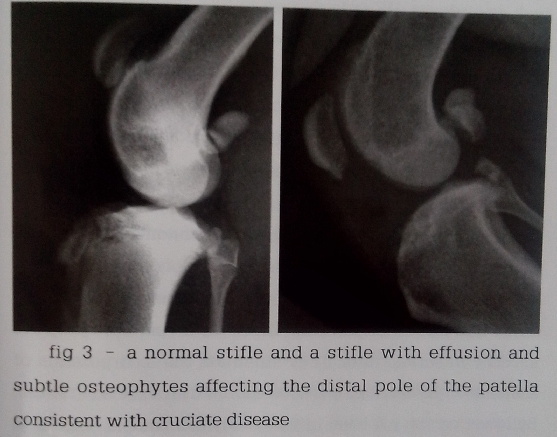
Hip dysplasia is a common radiographic finding,however the most common cause of pelvic limb lameness in dogs is cranial cruciate ligament (CCL) disease. In older patients lameness due to lumbosacral disease must also be considered as another major differential. In some cases wir.h complete CCL rupture there is often marked instability and the diagnosis is relatively straightforward by pe:rtorptiing cranial draw or tibial thrust tests. Partial tetiis aro easily overlooked, as the joint is often palpably st.able. Cruciatc,disease is often bilateral in nature cuid tin such case.s Lhere is no normal 'contralateral' comparison, making diagnosiseven more challenging. Accurate assessment of appiopriate radiographs for joint effusion and characteristic osteophytes(tig 3) can give the surgeon all the information lequired to make a diagnosis and proceed with corroctive surgery.
Carpal & Tarsal Injuries
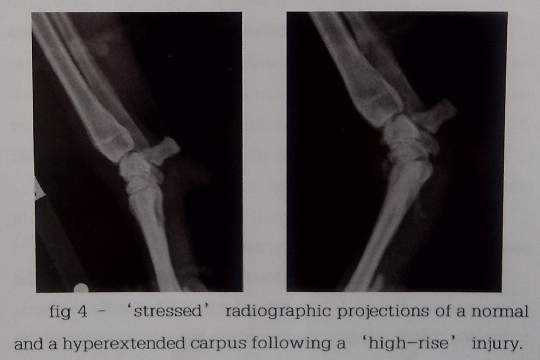
The carpus and tarsus are complex joints and a systematic approach to assessment of these joints will allow the surgeon to accurately assess which structures may havebeen damaged. Takirig radiographs with the limb held in
either valgus or varus 'stress' will aid in tlhe diagnosis of collateral ligament injury and likewise similar techniques can be used to demonstrate the presence of injury to the palmar and plantar ligaments in the thoracic and pelvic limb respectively. Appropriate management of distal lim:b joint injury is dependent on an accurate diagnosis. In cases of hyperextension injury (fig 4), the only effective treatment is arthrodesis of the injured joint due to the tensile forces created during weight bearing.
|
